
Ectopic Pregnancy After IVF: Signs, Risks, and What Happens When It Ruptures

Dr Mannan Gupta
Medically Reviewed by Dr. Mannan Gupta On June 11, 2026

You have done everything right — the injections, the retrieval, the transfer. You have waited, hoped, and finally seen those two lines appear. And then something starts to feel off.
An ectopic pregnancy after IVF is one of the most feared — and most misunderstood — complications in fertility treatment.
For couples navigating ectopic pregnancy after IVF in New Delhi, knowing the signs, understanding the risks, and having access to an expert team can quite literally save a life.
Key Takeaways
- Why ectopic pregnancy can still happen even after IVF embryo transfer
- Which patients are at higher risk — and the role your uterine lining plays
- The early warning signs, including one that almost everyone misses
- What a rupture looks and feels like, and why it demands immediate action
- The hidden danger of heterotopic pregnancy that most blogs never mention
- All available treatments and what they mean for your future IVF cycles
What Exactly Is an Ectopic Pregnancy — and Can It Really Happen After IVF?
Definition and Where It Implants
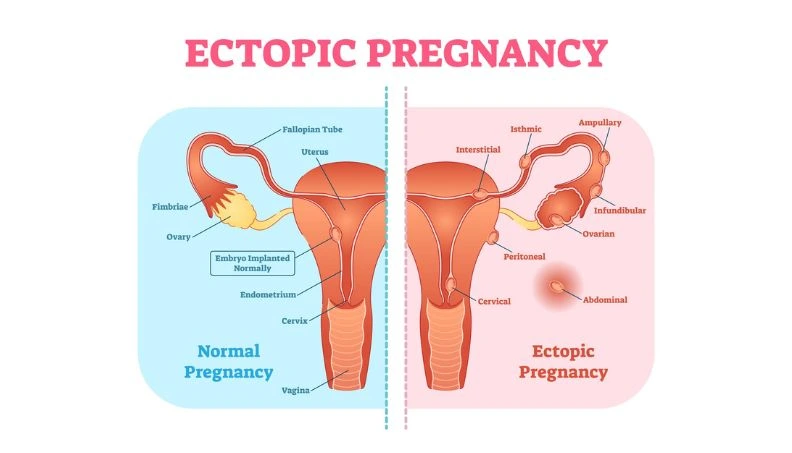
An ectopic pregnancy occurs when a fertilized embryo implants and begins to grow somewhere outside the uterine cavity.
The fallopian tube is the most common site, accounting for over 95% of cases. Less commonly, the embryo can lodge in the ovary, the cervix, or even within the muscular wall of the uterus near the tubal opening — a location called an interstitial or cornual ectopic, which carries particularly high risk.
Why IVF Doesn’t Guarantee Uterine Implantation
Many patients are surprised — and understandably confused — when an ectopic pregnancy occurs after IVF.
After all, wasn’t the embryo placed directly into the uterus? The answer is yes, but after the transfer, embryos can migrate.
In the hours and days following placement, a fluid current exists inside the uterine cavity, and in some cases an embryo can travel through the cornual opening and settle inside the fallopian tube, particularly if tubal damage exists.
How Common Is It in IVF Cycles?
Ectopic pregnancy occurs in approximately 1.4–5.4% of IVF cycles, compared to 1–2% in natural conception.
This elevated rate is not caused by IVF itself but rather reflects the underlying conditions — damaged tubes, endometriosis, and pelvic adhesions — that made IVF necessary in the first place.
The risk can vary significantly depending on individual factors, which is why understanding your personal profile matters deeply.
For couples seeking specialist-led IVF Treatment in New Delhi, a structured monitoring protocol from the very first cycle can make all the difference in detecting and preventing complications early.
Who Is at Higher Risk of Ectopic Pregnancy After Embryo Transfer?
Damaged or Blocked Fallopian Tubes
Women with a history of tubal surgery, pelvic inflammatory disease (PID), or a prior ectopic pregnancy carry significantly elevated risk.
Scarred or damaged tubes may be structurally altered in ways that make it easier for a migrating embryo to implant in the wrong location.
In some cases, when severe tubal damage is identified before IVF, a specialist may recommend surgical removal of the tube (salpingectomy) beforehand to reduce risk and improve IVF success rates simultaneously.
If you have been told you have damaged or obstructed tubes, it is worth understanding all available options — you can learn more about Blocked Fallopian Tubes Treatment in New Delhi and how early intervention can influence your IVF outcome.
Past Pelvic Infections and Endometriosis
Pelvic infections, even when treated years ago, can leave behind microscopic scarring that distorts tubal anatomy.
Endometriosis — a condition where uterine tissue grows outside the uterus — causes chronic inflammation and adhesions around the tubes and ovaries, subtly altering the environment in ways that increase ectopic risk. These are factors often identified at the time of fertility investigation.
Transfer Type and Embryo Stage
Research consistently shows that cleavage-stage embryo transfers (day 2–3) carry a higher ectopic risk than blastocyst transfers (day 5–6).
A blastocyst is a more developed embryo with a narrower window of implantation, giving it less time to migrate before it must attach. Transferring a single, high-quality blastocyst in a well-prepared cycle is currently the approach most supported by evidence for reducing ectopic risk.
Thin Uterine Lining and Its Role
This is a connection that most patients — and many general doctors — are unaware of. A thinner uterine lining is associated with a higher rate of ectopic pregnancy.
Research published in reproductive medicine journals demonstrates that patients with a lining above 7.6 mm on transfer day had significantly lower ectopic rates.
A well-prepared, receptive endometrium acts as a welcoming home that reduces the embryo’s tendency to settle elsewhere.
This is a modifiable, measurable factor your fertility specialist can actively optimize.
Dr Mannan IVF Centre
Experience world-class fertility care with Dr. Mannan Gupta at the Best IVF Centre in Delhi
What Are the Early Signs of Ectopic Pregnancy After IVF?
Pelvic Pain and One-Sided Cramping
One-sided pelvic or lower abdominal pain — particularly a persistent cramp on the left or right — is the most important early symptom of ectopic pregnancy. This occurs as the embryo grows within the limited space of the fallopian tube.
It is often dismissed as implantation discomfort or normal post-transfer sensations, which is precisely why it is missed.
If you feel cramping that is localized to one side and does not resolve, contact your fertility team the same day.
Unusual Bleeding After Embryo Transfer
Some spotting after embryo transfer is normal. But heavier bleeding, or bleeding accompanied by pain, is a red flag that must never be attributed to implantation bleeding without an ultrasound to confirm location.
An ectopic pregnancy can cause irregular vaginal bleeding as early as 6–8 weeks after the last period, and this can be deceptively light.
It is important to remember that IVF patients can experience more than one complication at once — if you are also experiencing bloating, nausea, or abdominal discomfort in the early post-transfer period, it is worth reading about OHSS After IVF: Symptoms, Prevention and When to Call Your Doctor, as distinguishing between these conditions early is key to getting the right care.
Shoulder Tip Pain — The Warning Most Patients Miss
Shoulder tip pain — a sharp or aching sensation at the very tip of the shoulder — is a sign of internal bleeding irritating the diaphragm, and it is one of the most serious early warnings of an ectopic pregnancy.
It has nothing to do with the shoulder joint itself. Many patients experiencing this symptom visit an orthopaedic or simply take a painkiller, unaware of its significance.
If you experience shoulder tip pain alongside pelvic discomfort after an embryo transfer, go to an emergency room immediately.
What Happens When an Ectopic Pregnancy Ruptures?
Why Rupture Is a Medical Emergency
A fallopian tube is a narrow structure never designed to accommodate a growing pregnancy. As the embryo develops, it stretches and eventually tears the tube — causing severe internal bleeding into the abdominal cavity.
A ruptured ectopic pregnancy is a life-threatening obstetric emergency, requiring immediate surgical intervention. Without treatment, it can be fatal within hours.
The Specific Symptoms of Rupture
Rupture typically causes sudden, severe pain in the lower abdomen — often described as a stabbing sensation that comes on without warning.
It is frequently accompanied by extreme dizziness or fainting, very pale or clammy skin, a drop in blood pressure, nausea, and an intense pressure or urge in the rectum. These symptoms indicate active internal haemorrhage and demand emergency medical attention.
The Critical Window to Act
Time is the single most important factor in a rupture. Every woman who has undergone an embryo transfer and develops these symptoms must be taken to a hospital immediately — do not wait, do not monitor at home, do not take painkillers and sleep it off.
The outcomes for women who reach emergency care promptly are excellent. Delay is the danger.
The Hidden Danger — What Is a Heterotopic Pregnancy?
When One Embryo Is in the Right Place and One Is Not
A heterotopic pregnancy is a rare but serious condition in which one embryo implants correctly inside the uterus while another simultaneously implants in the fallopian tube.
This is almost uniquely a complication of IVF because it typically requires multiple embryos to be in the reproductive tract at the same time. In the general population, heterotopic pregnancy is extremely rare — but in IVF, it occurs in up to 1% of cycles with multiple embryo transfers.
Why hCG Levels Can Be Misleadingly Normal
In a typical ectopic pregnancy, the beta-hCG hormone level rises more slowly than in a normal pregnancy — a key diagnostic clue. But in a heterotopic pregnancy, the normally implanted uterine embryo drives hCG levels that appear completely reassuring, masking the dangerously abnormal tube pregnancy.
This makes heterotopic pregnancy one of the most diagnostically challenging conditions in reproductive medicine.
How It Is Diagnosed and Why It Is Frequently Missed
Transvaginal ultrasound is the only reliable way to detect a heterotopic pregnancy, and it must specifically search beyond the uterine cavity.
Even experienced sonographers can miss a tubal pregnancy when a visible intrauterine sac reassuringly appears on screen.
This is precisely why IVF patients with any pelvic pain should have a thorough ultrasound that explicitly examines both adnexal regions — not just confirms an intrauterine sac.
How Is Ectopic Pregnancy After IVF Diagnosed?
The Role of Serial hCG Monitoring
After an IVF embryo transfer, beta-hCG blood tests are typically done at specific intervals — and crucially, it is the trend of rise, not the single number, that matters most. In a healthy intrauterine pregnancy, hCG doubles approximately every 48 hours.
When levels rise too slowly, plateau, or rise in an atypical pattern, this signals that the pregnancy may not be developing normally inside the uterus.
Doctors use what is called a “discriminatory zone” — a threshold hCG level above which an intrauterine sac should always be visible on ultrasound. If it is not visible at that level, ectopic pregnancy must be actively ruled out.
Transvaginal Ultrasound — The Gold Standard
A transvaginal ultrasound (TVUS) performed by an experienced sonographer at the right gestational age — typically around 5–6 weeks — can directly visualize an ectopic mass, detect free fluid in the abdomen (a sign of bleeding), and confirm or rule out an intrauterine sac simultaneously.
In IVF clinics, this scan is a scheduled part of the post-transfer protocol, which is one major advantage of undergoing treatment in a well-structured fertility centre.
What Are the Treatment Options — and Do They Affect Future Fertility?
Methotrexate — The Non-Surgical Option
For ectopic pregnancies that are diagnosed early, are small in size, and have not ruptured, methotrexate injection is a safe and effective non-surgical treatment.
Methotrexate is a medication that stops the rapidly dividing cells of the ectopic tissue from growing. The pregnancy is then gradually reabsorbed by the body over several weeks.
It requires close follow-up with serial hCG measurements until levels reach zero. Not everyone is a candidate — it requires no signs of rupture, no significant internal bleeding, and hCG levels typically below 5,000 mIU/mL.
Laparoscopic Surgery — When and Why
When methotrexate is not appropriate, or when rupture has occurred, laparoscopic (keyhole) surgery is the definitive treatment.
A surgeon can either remove the ectopic pregnancy from within the tube (salpingostomy) or remove the affected tube entirely (salpingectomy).
Modern laparoscopic surgery is minimally invasive, involves small incisions, and typically requires a recovery of 1–2 weeks. The remaining tube, the uterus, and ovaries are preserved wherever possible to protect future fertility.
Once recovery is complete, many patients are ready to consider their next steps — if you are navigating the emotional and practical side of moving forward, our guide on what to do after a failed embryo transfer addresses many of the same questions that arise after an ectopic pregnancy as well.
Can You Do IVF Again After an Ectopic Pregnancy?
Yes — and this is the hopeful truth that patients deserve to hear clearly. A history of one ectopic pregnancy does not close the door on future IVF cycles or on a healthy pregnancy.
More than half of women who experience an ectopic pregnancy — including after IVF — go on to have a successful, healthy baby.
Your fertility specialist will review the underlying causes, adjust the protocol if needed, and plan your next cycle with full awareness of your history.
It is also worth knowing that a pregnancy achieved after an ectopic history may require additional monitoring — our earlier guide on High-Risk Pregnancy After IVF: Precautions covers exactly what to expect and how to stay safe in subsequent cycles.
If you are undergoing IVF and have any concerns about ectopic pregnancy risk, or if you have experienced a prior ectopic and want guidance before your next cycle, Dr. Mannan Gupta and the team at Dr. Mannan IVF Centre in New Delhi are here to help.
Final Thoughts
Ectopic pregnancy after IVF is a complication that is real, serious, and — when caught early — entirely manageable.
The most important protections you have are awareness of the symptoms, access to serial hCG monitoring, and a timely ultrasound from an experienced team.
Shoulder tip pain is not a muscle problem. One-sided cramping after embryo transfer is not normal discomfort to push through.
Slow-rising hCG is not something to watch and wait on at home. These are signals that require prompt medical attention.
With the right care team and the right information, ectopic pregnancy does not have to be the end of your IVF journey — for most women, it is a detour, not a dead end.
Frequently Asked Questions
1. Can an ectopic pregnancy happen even after a single embryo transfer?
Yes, it can, though the risk is lower with a single embryo transfer than with multiple embryos transferred simultaneously. Even a single embryo can migrate from the uterine cavity into the fallopian tube after being placed. The risk is significantly influenced by the condition of the fallopian tubes rather than the number of embryos alone.
Single blastocyst transfers in women with healthy tubal anatomy carry a low but non-zero ectopic risk, which is why early hCG monitoring and ultrasound remain essential in every IVF cycle.
2. Does having an ectopic pregnancy mean my IVF failed?
Not entirely. While an ectopic pregnancy is not a successful outcome, it does confirm that fertilization occurred and that the embryo was capable of implanting — which are positive biological indicators. The goal is to understand why it implanted in the wrong location and adjust the approach for the next cycle. Many women successfully achieve uterine pregnancies in subsequent IVF cycles after an ectopic, particularly when the underlying risk factor is identified and addressed.
3. How quickly can a rupture happen after an ectopic pregnancy is detected?
There is no fixed timeline, and this is precisely what makes ectopic pregnancy dangerous. Some ectopic pregnancies rupture as early as 6 weeks of gestation; others may persist to 10–12 weeks before rupturing. The rate of growth of the ectopic tissue, the location of implantation, and the structural integrity of the tube all influence timing. This unpredictability is the clinical reason why a confirmed or suspected ectopic pregnancy is always treated as urgent — waiting and watching without specialist oversight is never safe.
4. What should I do if I'm between monitoring appointments and I develop pain?
Do not wait for your next scheduled appointment. If you experience sudden pelvic pain — especially one-sided — shoulder tip pain, dizziness, or any bleeding that concerns you, contact your fertility clinic immediately or go directly to an emergency department. Tell them you have recently had an embryo transfer and that ectopic pregnancy needs to be ruled out. Early presentation is the single most powerful factor in a safe outcome.
5. Is it safe to use methotrexate for ectopic pregnancy and then try IVF again?
Yes, methotrexate treatment for ectopic pregnancy does not permanently affect fertility or IVF candidacy. However, after methotrexate, it is essential to wait until hCG levels have completely returned to zero and your specialist confirms that the body has fully recovered — this typically takes several weeks to months. Most fertility specialists recommend waiting at least three menstrual cycles before the next embryo transfer to ensure the uterine environment is fully optimized for implantation.
